
Interview with Dr. Steffen König, head of Clinic of Trauma and Reconstructive Surgery, Märkisch-Oderland Hospital, Strausberg, Germany
Located 30 km east of Berlin and 30 km west of the Polish border, Strausberg is the largest town in the district of Märkisch-Oderland. In 2000, in order to meet population’s demands for healthcare, the Märkisch-Oderland Hospital merged clinics in Strausberg and Wriezen, creating a modern hospital network.
In 2008, in addition to the Clinic of Trauma and Reconstructive Surgery, the hospital of Strausberg created the Clinic of Trauma and Reconstructive Surgery under the leadership of Dr. König. The clinic has since continued to develop its expertise by focusing on the specialized care of patients who suffered of acute accidents.
One specialty of the clinic is the treatment of spinal injuries with minimally invasive surgery techniques, the department recently acquired an OEC 3D C-arm for high precision intraoperative 3D imaging.
Dr. König shares with us what was important when selecting a new 3D C-arm and how his hospital integrated the OEC 3D C-arm during orthopedic traumatology procedures.

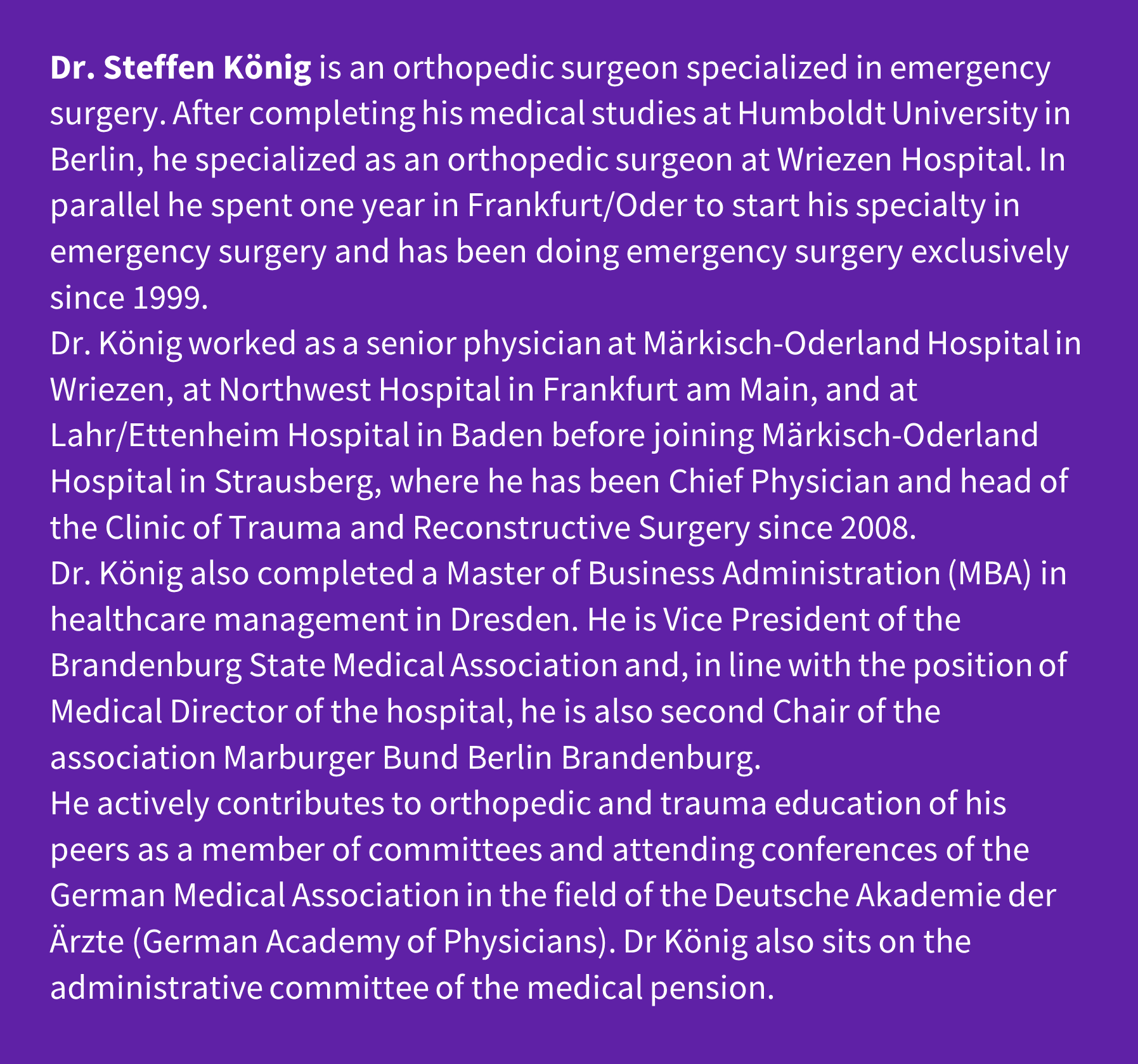
Dr. König and Dr. Peuthert operating a patient knee & Dr. Peuthert checking 2D image on OEC 3D workstation.
Dr. König can you explain to us the activity of the Clinic of Trauma and Reconstructive Surgery at Märkisch-Oderland Strausberg Hospital?
The district of Märkisch-Oderland has approximately 200,000 inhabitants. Healthcare for this population is covered by four hospitals. Three of these four hospitals are in our group: the hospitals in the cities of Wriezen, Seelow, and Strausberg.The Märkisch-Oderland Strausberg Hospital covers various clinical activities including orthopedic surgery, directed by one of my colleagues, as well as traumatology and reconstructive surgery which I lead.The primary spectrum of our activity is emergency surgery of age-related trauma due to the demographic evolution of our district. Thus, we treat a very large number of fractures of the upper leg, proximal to the hip joints, as well as emergency surgery of big joints such knee and spine.Our clinic is approved for the process of consultation of accident, but not for treatment of severely injured patients. These patients are addressed to the emergency hospital in Berlin.The staff includes our senior surgeon, Dr. Peuthert, two specialists, three assistants and myself, head of the clinic. We can manage patients through the community health center.One of our operating room is actually an emergency room. It is currently managed by a senior physician, a deputy, and an assistant physician. The clinic has 30 beds, including beds that we can use in intensive care and intermediate care.
As a trauma specialist, what is your experience with surgical and 3D imaging, and how did you choose OEC 3D?
I started working with 3D C-arms in 2004 when I was senior physician in emergency surgery at the Northwest Hospital of Frankfurt am Main and later in the Hospital of Lahr/Ettenheim where I gained experience and saw the benefits in 3D imaging and also used navigation systems with the first generation of products we used from Siemens.

Dr. König checking patient draping before running 3D acquisition.
When I joined Märkisch-Oderland Strausberg Hospital, we saw the need to acquire a 3D C-arm without navigation given the type of procedures we carry out in our department.
Initially, in 2008, we opted for the Ziehm 3D C-arm which we used for several years with good 2D imaging, but some limitations in the 3D image quality.
In 2022, we started tendering again for a new 3D C-arm, and after testing C-arms available on the market, I was pleasantly surprised by the image quality of OEC 3D.
Through my experience in trauma surgery, I tested several types of C-arm designed for 3D imaging. I have found that C-arms rotating more than 180 degrees provides superior 3D image quality.
During the renewal process, as we have relatively small operating rooms, I wanted to verify that the new 3D C-arm could fit in the room for different trauma procedures we do. We found that the size of OEC 3D is just the right. Initially we had some positioning challenges with upper leg fractures close to the hip joint because there is relatively little space. We also had to rethink a few things in terms of setup, but after the initial phase we now have an easy workflow in 2D and 3D imaging. The volumetric 3D images are produced relatively quickly in the intraoperative workflow.
With OEC 3D I believe we get the right balance of excellence in 2D and 3D imaging with a reasonable C-arm footprint even for our small operating room.
“Overall we can say the OEC 3D C-arm is easy to operate in 2D and 3D imaging and it provides us very good image quality for our procedures. These are the reasons why we decided to choose it for our daily practice.”
Can you tell us which procedures you need 2D/3D imaging for, and what are the advantages?
In general, there is no such thing as emergency surgery without 2D/3D imaging. We use 3D imaging in about 5 percent of the surgical procedures we perform. For our other procedures we only use 2D imaging. This is mainly due to our concern for radioprotection. We use 3D imaging only when needed.
Considering the relatively small operating room we have; we cannot have one C-arm for 3D and another C-arm for 2D imaging. In addition, bringing the device in and out requires a certain amount of logistical effort that the OR staff wouldn’t appreciate. We use OEC 3D for everything: 2D and 3D imaging.
In our clinic we do about 20 tibial plateau fractures per year and another 20 tibial head fractures per year with 3D imaging. Tibia fracture reduction is one of the most complex procedures in traumatology. The volumetric images give us information on the anatomy behind the knee, that is difficult to perceive with 2D projection images.
So, my main indications for the use of OEC 3D for 3D imaging includes the surgery of the fracture of the tibial plateau at the level of the knee and ankle particularly when implying bone fusion. We also use 3D imaging for procedures of pelvic repair in geriatric patients. It is a procedure we performed with pelvic screws and cementoplasty. I check in the volumetric images, that the implants are in a good position. In spine surgery, particularly with kyphoplasty, sometimes I am not one hundred percent certain with 2D imaging, of the locations where the cement has flown out. I use 3D imaging in order to check that the cement doesn’t go toward the spinal nerve and toward the spinal cord canal. It is fairly easy to correct after checking the 3D images. I also use 3D imaging in very complex fractures of the radius. Surgery of the elbow tends to be technically difficult, and 3D imaging provides more information to get a better idea on how to proceed.
The advantage for me to do intraoperative 3D imaging is simply to verify that I have reduced the fracture in an anatomically correct manner and that the screws are not too long. These are decisive advantages for me.
Starting 3D collision check on OEC 3D.

In the past, after doing the post operative CT scan of pelvic screw placement, we actually did have to correct the surgery. Obviously, I would not have to do that anymore, because we can do 3D imaging during the surgery. That’s the better solution.
I consider that doing intraoperative 3D imaging contributes towards minimizing the cost of the surgery. Revision surgery planned after a CT scan is requested because the patient feels pain costs money. When patients are in the hospital for a certain time it becomes uneconomical.
The goal of OEC 3D, with 3D imaging, is to be able to identify problems immediately and intraoperatively to avoid repeating interventions.

3D acquisition on going at 91% completion, projection images displayed on OEC 3D Touch View and Workstation.
Did OEC 3D require a special setup in the operating room or different set up for each procedure?
By experience I know that you should never start to operate and then look later at how to take X-ray images.
Instead, we need to anticipate how to position the C-arm to get the working space needed during the surgery, sometimes you need to compromise in order to get the information you have to get.
For example in 2D imaging, I like to use the retrograde intramedullary nail fixation technique for humerus fracture reduction with freehand tightening.
Patient lies in lateral decubitus, and in order to take profile views of his humerus we need to position the X-ray tube and the detector of the C-arm in the rainbow configuration, over the table. However, for this procedure we also need oblique views. We figured out how to position the patient far at the head end of the table and far away from the side of the table in order to do profile and oblique views in a comfortable way. With this setting we just sweep back and forth and move the C-arm along the table to get more anatomical coverage.
For 3D imaging, we didn’t encounter major difficulties. For procedures on the lower extremities we had to work more on the patient set up. We are used to positioning the contralateral leg outward and that’s a bit tight when working toward the knee. In that case, we prefer to stretch the leg out lengthwise, and we accept the loss of image quality we might get from the attenuation of the X-ray beam from the contralateral leg. But as said, we figure it out before starting the surgery and it is not an issue.
How do you use OEC 3D imaging protocols and acquisition modes during surgery?
When doing 2D imaging, we select the imaging protocol depending on the anatomy. We work on orthopedic or spine imaging profiles. We set up OEC 3D to low dose mode as it boots up and rarely change the settings as the system adapts automatically in real time. We like the image quality we get with this set up in 2D.

When doing kyphoplasty, we also like to use the C-arm angulation memorization function. Once we identified the hip oblique views, we store the angulation values and recall them. That’s valuable for the staff and the learning curve has been relatively quick.
We generally only run one 3D scan per patient for radiation exposure reasons. After reduction of the fracture and securing the osteosynthesis material in place, we run a 3D scan before we do the final osteosynthesis. Sometimes, if the screw lengths have to be verified, we perform another 3D scan. It is also the case if the patient suffers from discitis and we are trying to repair and shape the vertebrae, a second 3D scan can allow us to check whether the bones are in the correct position. The 3D scan is generally performed before the final implant is inserted during the procedure or at the end of the procedure.
We run 3D acquisition in High Definition (HD) mode, and we activate the Metal Artefact Reduction (MAR) function if needed.
“The positioning of the C-arm is fairly easy without dose as we like to use the 2 laser aimers to adjust the C-arm detector over the anatomy of interest.”
When we run the 3D acquisition scan, the anesthetist stays in the corner of the room so that he can see the patient, and I usually stay at a safe distance of four meters from the C-arm. I do this because when I run the 3D scan, I always look at the images of projection that are acquired in real time because this loop of images provides me with additional information. For image review, I like to manipulate the 3D images on the 3D volume viewer of the workstation myself. I know what I am looking for and I can review the information directly using the multi oblique view function without asking anyone. The large size of 3D volume 19 cm x 19 cm x 19 cm is an advantage for our procedures. In particular it is interesting when we are placing pelvic screws. The 3D volume we had before with our previous C-arm was definitely not sufficient. I am really interested to get volumetric images of the sacrum, to check how the wires are positioned, how the screws could be placed later on during the procedure. OEC 3D user interface and 3D workflow were new to me and to our team but the learning curve was quite fast as the design is intuitive. Our OR staff are running the 3D collision check, under supervision of surgeons and guided by the 3D Setup Assistant.
The OEC 3D C-arm is rather compact for a 3D C-arm, and its carbon fiber C-arm is a good size for our work. It is the type of design we will need more and more in the future, with an image quality that looks more like that of an intraoperative CT scanner. OEC 3D C-arm is easy to operate and it is very good quality. These are the reasons why we decided to choose it for our daily practice.

The statements by GE HealthCare customers described here are based on their own opinions and on results that were achieved in the customer’s unique setting.
Since there is no “typical” hospital and many variables exist, i.e. hospital size, case mix, etc., there can be no guarantee that other customers will achieve the same results. JB25821XX